When I found out my platelets were below normal this year, I went through a variety of emotions, but absent was fear. I was in remission for four years and three months, surely I could do it again. After all, I was in the same hospital system seeing a colleague of my favorite doctor, I thought for sure it would be smooth sailing.
I was wrong.
I had to push for weekly CBCs, not being taken seriously about how quickly my platelets could crash. Two weeks later, I dropped from 129,000 to 53,000. I was put on Prednisone, the drug that destroyed my body and left lasting damage. The doctor assured me it was only a temporary treatment. I thought once ITP showed him what it was capable of, he would take what I say seriously.
Again, I was wrong.
My platelets started to rise, and stayed stable on high doses, but that drug was killing me. I kept asking my doctor about Rituxan, my life saver. The one drug that Dr. Ahn and I knew would put ITP into remission. It dangled in front of me like a carrot. He again refused to prescribe me Rituxan, he was perfectly fine leaving me on the drug that was destroying my body. The doctor kept saying, “Rituxan is not a benign treatment.”
I was in self-preservation mode at this point, getting worse as the weeks went by. I found my new physician, who knew Dr. Ahn and his research. I opened up to him about my desire to use Rituxan and he didn’t string me along. Instead, we created a plan based on how I wanted to fight ITP.
Rituxan worked, again.
I spent four weeks watching as the infusions started fighting back. I also was slowly feeling like myself, regaining my identity beyond just being “sick”.
After all of this, my emotions are still a bit raw. However, I am reminded that Dr. Ahn gave me the tools to continue to fight this disease well after he retired. It wasn’t just preparation for a single victory against ITP, but a lifetime of fighting back.
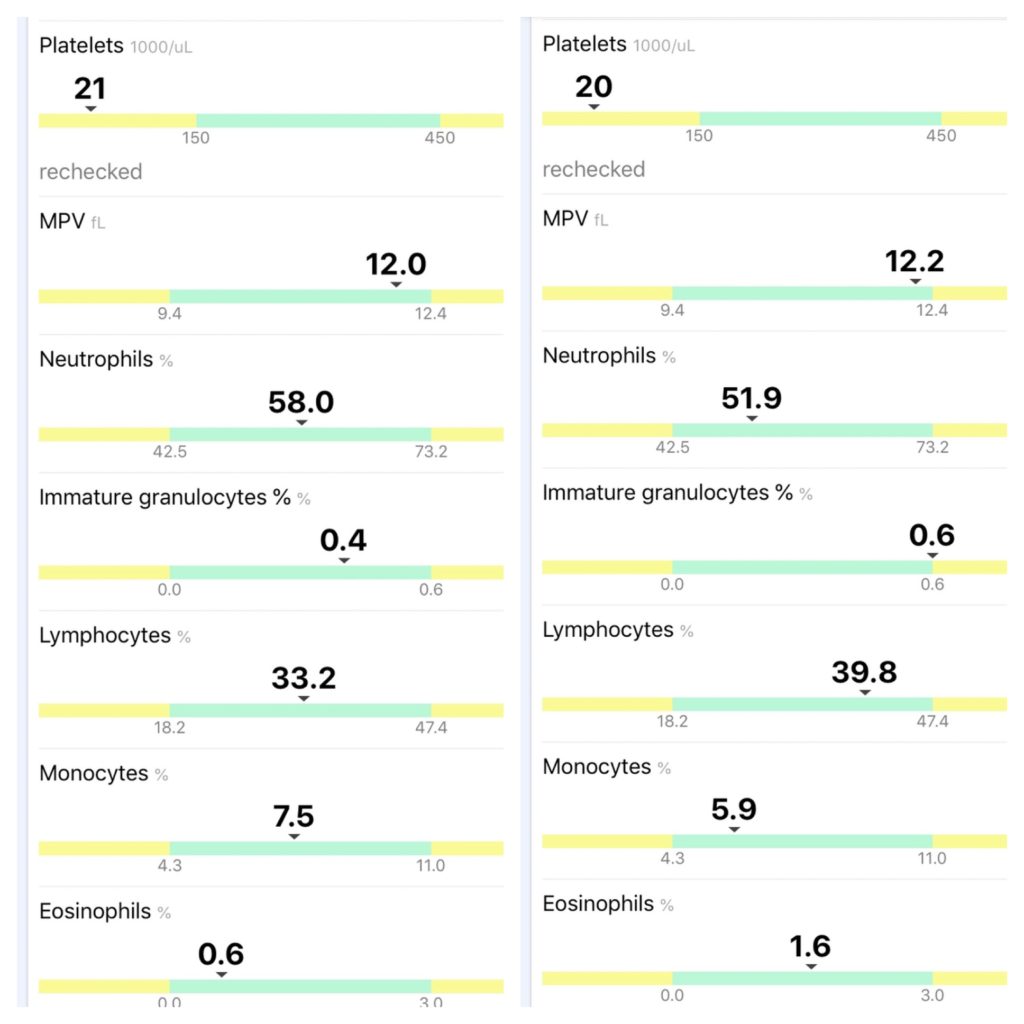
The photo above shows my last two CBCs. I was at 94,000 platelets when I had my first Rituxan infusion on 7/1, and before my second infusion this past Monday (7/8), I went up to 100,000! I was killing off around 12,000 platelets a day before treatment, so this was extremely impressive.
I am feeling pretty good despite the mild headaches, constipation, fatigue, and lack of appetite. Those things really don’t bother me when I know my B-cells are being suppressed!
My next infusion is Monday, and I’ll have another CBC before treatment. I am curious to see where my platelets will be at the half-way mark. I’ve noticed my purpura fading, I haven’t developed any new bruises and I have no brain fog. So far, a night and day difference.
Some other good news: my nurse Jen was able to tap my wrist for the infusion, which saved me from having to hold my arm straight for a few hours. I also was administered 100mg of IV steroids in addition to Benadryl and Tylenol as pre-meds. I infused pretty quickly, from 10 am to 1:15pm, with no reaction. The only thing I don’t like about my wrist is the burning in my arm after Benadryl. It hurts for about 15 minutes and then subsides. I also have to be careful that I don’t let anything touch the area for 24 hours after, because it is tender. I usually wear my Apple Watch on my left wrist, but have to keep it off while the area heals.
That’s the update for now, I am happy with how things are progressing and ready for infusion three. #PlateletsUp
I’m home from my first Rituxan infusion, only three left to go!
While I’m smiling, I need to be brutally honest. Today was hard, the smile is put on. I’m tired, stressed, and I had another massive emotional rollercoaster caused by our broken healthcare system. I almost didn’t have my infusion today.
It was my first time taking an infusion at the elbow. While I had to focus on keeping my arm straight, it hurt a lot less and didn’t burn!
First, upon my arrival to the infusion center my authorization was not in the system. Instead of calling upstairs to get the information, they made me go upstairs to find the employee responsible. Why it couldn’t have been handled by a phone call I’ll never know. Just another part of the process where the systems and staff don’t seem to have an open line of communication. Insurance issues are handled in an entirely separate department and no one knows how to navigate it outside of a few people. Thankfully, the problem was fixed with a phone call down to the infusion center from the authorization staff.
When signing all the paperwork to do Rituxan last Tuesday, I had to take a pregnancy test to process the orders. It took my doctor a good ten minutes of navigating the EHR system to determine which of the tests was needed for Rituxan. At no point was a Hepatitis B panel shown, but apparently I needed that too. Unfortunately when I went to infuse today, my treatment was almost cancelled because I didn’t have the panel done. It wasn’t discovered until the Pharmacy was prepping my infusion. My amazing nurse got my doctor on the phone (he’s out on vacation) to override the testing requirement so we could get the prescription processing. She ended up drawing blood and everything came back fine.
At the time this all went down, I finally broke down and cried. This disease has been a constant source of unrelenting stress since March. I honestly never anticipated having this much trouble when ITP came back. Pair that with not sleeping and feeling generally miserable because of crashing platelets, I couldn’t hold in my frustration any longer.
While I tend to handle my disease with sarcasm, humor, and witty banter, I am still human with raw emotions. The system is not designed for rare disease patients, especially ones who are using off label therapies. We are forced to micromanage care, and anytime you look away, you risk someone else dropping the ball. Most of the time, those people are not the ones directly caring for you (like doctors or nurses), so it makes advocating for yourself much more difficult.
I absolutely hate having to be assertive, direct, and at times downright demanding to get what I need to battle ITP. I want to find creative solutions to the problems all of us rare disease patients face. Every time I’ve shared these bumps in the road, patients tell me their horror stories. I know we are not alone, but it seems like the system temporarily corrects itself for one of us, then goes right back to operating under broken processes. At the end of the day, this helps no one, because the cycle continues.
I hope that after all my infusions are finished and I am back in remission, I can work with payers, hospital systems, EHR companies, legislators and rare disease groups to fix a lot of these issues. There’s no sense in dismissing them once my treatments are over, because I will eventually be back in the system when I come out of remission again. I also want to turn negatives into positives. I want my challenges, problems, and pain points to help inspire change.
Now on to some interesting things about today’s infusion:
I had a reaction an hour in, complete with itchy eyes, throat and ears. I became flushed while my nose got stuffy. They had to stop the infusion and administer more Benadryl plus IV steroids. I had pre-meds of Benadryl and Tylenol, but no steroids. That’s likely what caused my allergic reaction (it was similar to what I experience with cats). For the next three infusions, I am going to ask for the steroids as pre-meds too.
My platelets went from 169,000 to 94,000 in 6 days. I am destroying them rapidly, so I am anxious to see how quickly Rituxan will work.
Food already tastes a little bland, but I’m hoping that will help me lose the 10lbs I gained from steroids!
Now that infusion one is finished, I am anxiously awaiting next Monday. Keeping my fingers crossed that the rest of the process is smooth from here on out. I appreciate the compassion shown by my nurse today. She went above and beyond to advocate for me when I felt defeated. She made it happen, and for that I am eternally grateful.
On Monday 7/1, I’ll be repurposing Rituxan for Immune Thrombocytopenia for a second time. The goal is to put me back into remission for an extended period of time. When I used Rituxan at the end of 2014, I had a remission period over four years. I’d like to think we will be able to achieve similar results this time around.
Rituxan is a chimeric monoclonal antibody targeted against the pan-B-cell marker CD20. In plain English, it targets B-cells by going after CD20 which is expressed on the surface. Ultimately, after multiple blood tests and positive results from immunosuppression by steroids, we were able to figure out my B-cells were responsible for destroying my platelets. By shutting them down using Rituxan, I am able to maintain a normal platelet count.
The first test I received is Anti-Nuclear Antibody (ANA) which came back positive and indicates autoimmune activity. We also tested for Lupus, Rheumatoid Arthritis, and Sjögren’s Syndrome among others. I ended up also testing positive for SS-B antibodies, further confirming autoimmune activity. Another great marker: I respond very well to immune suppression with Prednisone. All of these factors collectively helped my doctor come to the conclusion that I had chronic Immune Thrombocytopenia and I was destroying platelets via my B-cells. I never had a bone marrow biopsy because when I am on high doses of Prednisone, my platelet count returns to normal. There is nothing to indicate that I have any issues with platelet production in my bone marrow.
Because of this, N-Plate and Promacta would not be the right treatment for me. I could stimulate platelet production, but my B-cells would destroy those platelets as well. Ultimately, the idea is to stop the process of platelet destruction. That’s how I came to the decision to use Rituxan in 2014, and why I advocated so hard to use it again this time.
So now I begin the process of making myself an N-of-1 example of how Rituxan can help ITP patients with B-cell led destruction of platelets. We will collect a CBC before each of the four infusions to track progress. I am currently on no medication for my platelets after I finished my Dexamethasone pulse last Monday (one week before my first infusion).
Besides chasing remission for a second time, I had an inordinate amount of trouble getting insurance to approve this treatment. We must see to it that Rituxan become an on-label therapy for Immune Thrombocytopenia, especially since patients with B-cell led destruction of their platelets do not have an FDA-approved treatment.
Acknowledging the clinical diversity of ITP is a must, especially with multiple drugs on the market and more in development. There is no one size fits all treatment for ITP, and what works for me may not work for another patient. Gathering treatment data and comparing it with ANA tests will be a great way to dissect some potential remission patterns in patients.