When I found out my platelets were below normal this year, I went through a variety of emotions, but absent was fear. I was in remission for four years and three months, surely I could do it again. After all, I was in the same hospital system seeing a colleague of my favorite doctor, I thought for sure it would be smooth sailing.
I was wrong.
I had to push for weekly CBCs, not being taken seriously about how quickly my platelets could crash. Two weeks later, I dropped from 129,000 to 53,000. I was put on Prednisone, the drug that destroyed my body and left lasting damage. The doctor assured me it was only a temporary treatment. I thought once ITP showed him what it was capable of, he would take what I say seriously.
Again, I was wrong.
My platelets started to rise, and stayed stable on high doses, but that drug was killing me. I kept asking my doctor about Rituxan, my life saver. The one drug that Dr. Ahn and I knew would put ITP into remission. It dangled in front of me like a carrot. He again refused to prescribe me Rituxan, he was perfectly fine leaving me on the drug that was destroying my body. The doctor kept saying, “Rituxan is not a benign treatment.”
I was in self-preservation mode at this point, getting worse as the weeks went by. I found my new physician, who knew Dr. Ahn and his research. I opened up to him about my desire to use Rituxan and he didn’t string me along. Instead, we created a plan based on how I wanted to fight ITP.
Rituxan worked, again.
I spent four weeks watching as the infusions started fighting back. I also was slowly feeling like myself, regaining my identity beyond just being “sick”.
After all of this, my emotions are still a bit raw. However, I am reminded that Dr. Ahn gave me the tools to continue to fight this disease well after he retired. It wasn’t just preparation for a single victory against ITP, but a lifetime of fighting back.
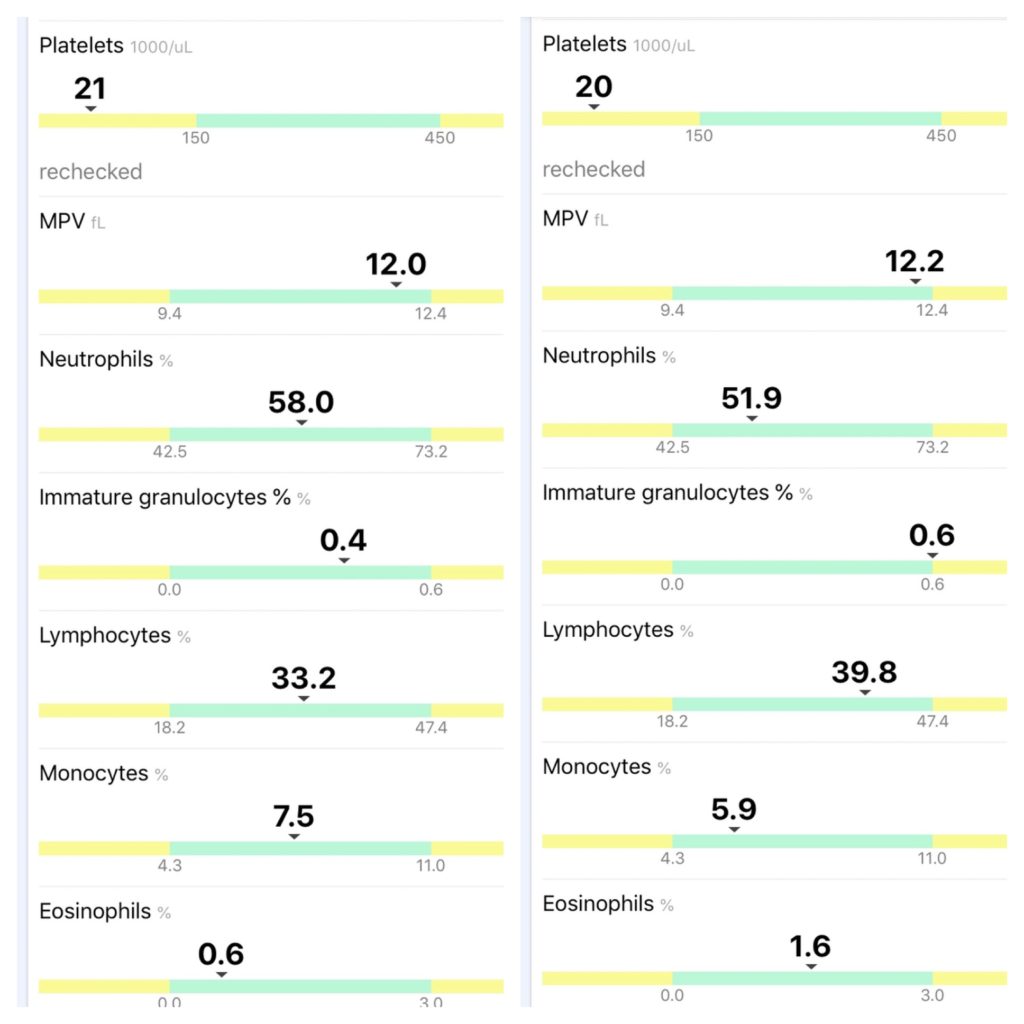
So here I am, in remission.
The doctor didn’t listen, so I found one who did.