Friday I went through my first round of Rituxan to attempt to treat Immune Thrombocytopenia Purpura. My decision came after 6 months of using high doses of Prednisone and failing to keep my counts above a safe level. The decision was not easy, the discussion with my doctors leading up to the final “ah-hah” moment was lengthy. Rituxan is not FDA approved for treating ITP (it is used for Non-Hodgkin’s Lymphoma), but it was approved for Rheumatoid Arthritis in 2006. My doctors suggested I consider it, I was scared at the idea but I ventured out to find out as much as I could.
I connected with multiple ITP patients online to discuss their experiences with the drug, as well as conducting my own research before talking to my doctors. This was out of the ordinary for me as I’m still new to the Rare Disease community. But I felt very empowered being able to hold a detailed scientific discussion about the pros and cons of “experimental medicine”. I read everything I could about reactions, response time and the biology behind the drug itself. Yes, the day after treatment I had cheese. I swear, I was craving it! Must have been the mice protein getting to me.
However, to the outside world, my decision was reckless. People were quick to declare me crazy, tell me I was poisoning myself, handing me cards to “healers” and nutritionists. Even going as far as telling me I am selling out to Big Pharma. Here’s a little hint: “Big Pharma” saved my life.There aren’t a lot of adults with chronic ITP in the world. Especially not like me. I’m not here to debate the existence of cures for disease, as I know there is no cure for ITP as the human immune system is a very large mystery. I am grateful that Big Pharma exists, and that they have the money and brain power to create options for me like Rituxan. If I am lucky, I will be one of those fortunate people who enjoys a period of remission from my disease.

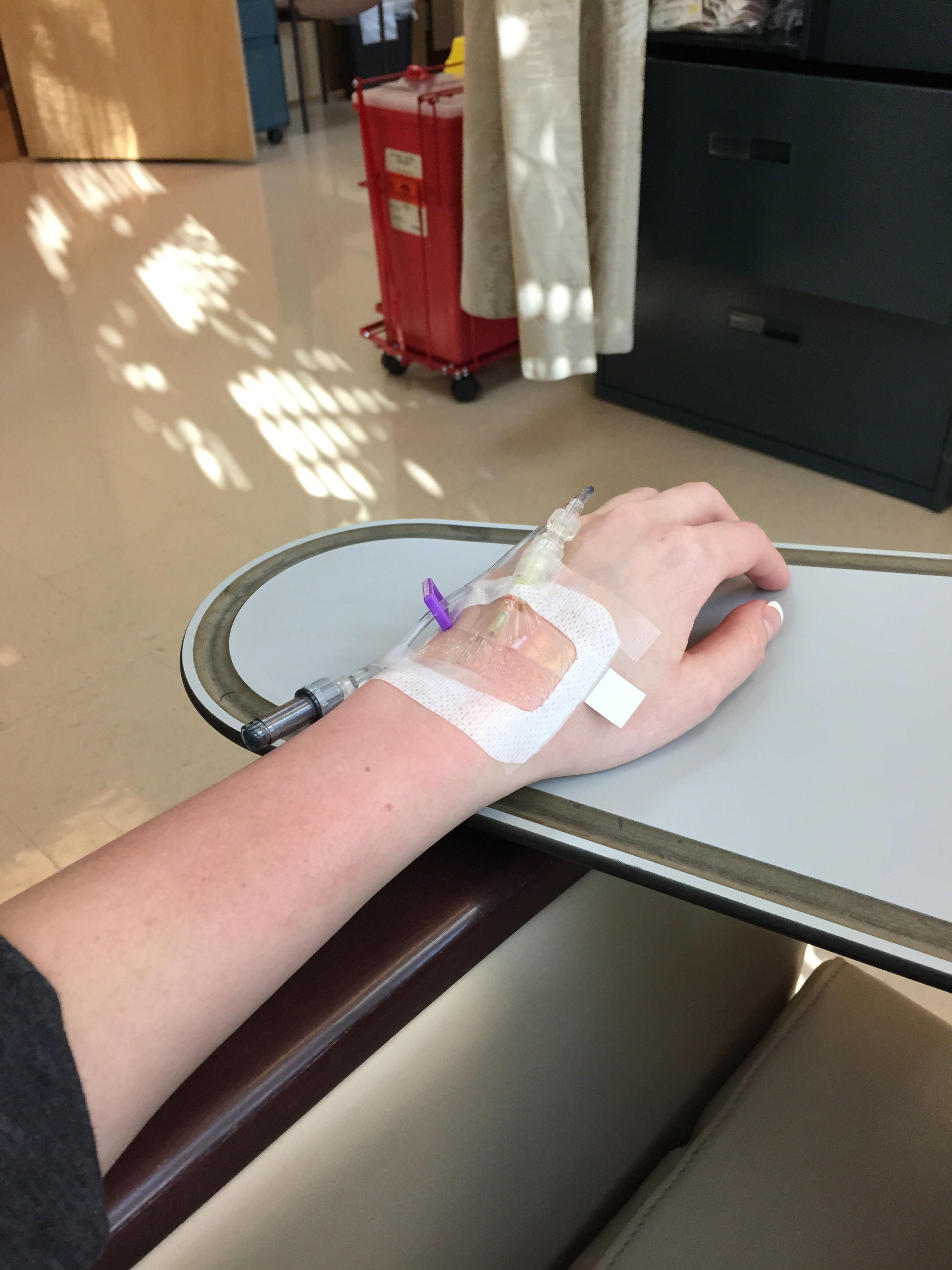
This hurt a lot less than anticipated
If Rituxan works, I am taking my story to the manufacturers of the drug to request that they pursue more studies for ITP patients. I am also going after Congress to push for improvements and edits to the Affordable Care Act, something that needs to happen for all rare and chronic disease patients. Our treatments and daily medications are expensive. There is no reason someone should consider whether or not to do a treatment based on cost. We should be making decisions based upon scientific knowledge, communication with other patients and self-driven research.
As my treatments continue over the next month, I expect to continue to be judged by the outside world. I will hear the whispers of how dangerous this is, how “stupid” I am to be killing myself with harmful chemicals and so on. The truth is, unless you step into the ring and face an opponent that cannot be beat, you cannot judge! This is my fight, I’m choosing to share it in hopes that maybe someone else stumbles along and will feel less alone.
Here I am as the Benadryl kicked in. My poor face was finally getting rid of the acne, and then I had to go back to 60mg of Prednisone.

If you are an ITP patient, caregiver or work in medicine, my advice to you from my war is to help keep open minds for everyone involved. My family, boyfriend and close friends were intimidated by the idea of “chemotherapy”. I even felt a little panicked after a while! So I sat down and started exploring, then I went back to everyone and said “I’m doing Rituxan!” It was a shock at first, but when I explained my research, what I had heard from other patients and what options I had, I felt that this was my best line of treatment.
For hematologists- it is important that you encourage your patients and their caregivers to look at the medical background surrounding Rituxan. It wasn’t so scary once I understood it is a monoclonal antibody against the protein CD20, not traditional chemotherapy. On the other hand it was also important that I was aware that reactions during infusion are serious and must be dealt with swiftly.
Bring on round 2!